Head to Toe: Naming of Prominent Skin Calluses in Muslim Populations

Introduction: Anatomical Namesakes
There are 169 well-known documented anatomical features in the human body ranging from the Adam’s Apple to the Zonule of Zinn. Our research has yet to conclude a definitive process on how each of these features received their eponymous designations. With the exception of those structures named after religious or mythological characters (e.g. the Achilles Tendon), most anatomical structures are named after white European and American males (including nine female body parts). Furthermore, the methodology for claiming and naming anatomical structures is not clearly defined, is it simply a “first come, first serve” or “first to document, first to claim” sort of situation? Or were they all the result of significant anthropometric/anthropological anatomical study?
It is interesting to note that many of these structures were named during the 17th to 19th centuries after the European Renaissance. Unfortunately, no structure is commonly named after any of the renowned Muslim/Arab anatomists such as Al Razi (Rhazeus: 854–932 CE), Ibn Sina (Avicenna: 980–1037CE) and Ibn Al Nafis (1213–1288 CE) who were pioneering anatomy and practicing medicine over a millennium before.
For example, Al Razi described the details of the Circle of Willis, the arterial circle located at the base of the brain named after English physician Dr. Thomas Willis, over 700 years before Willis was even born.
Another Arab Muslim scholar, Ali Ibn Abbas (Haly Abbas 930–994 CE), wrote his medical encyclopedia Ketab Kamel Al‐Sena‐a Al‐Tebiah (The Complete Art of Medicine), also known as Al‐Ketab Al‐Malki (The Royal Book), over half a millennium before the Renaissance. The anatomical section of this seminal book was the main source of anatomical sciences in both the Eastern and Western world for over a century. Ibn Abbas named six cranial bones: two squared parietal bones (Al‐Yafokh), two triangular temporal bones (Al‐Janibain), the frontal bone (Al‐Jabha) and the occipital bone (Azm Moa’akerat Al‐Ra’as). Moving from head to toe, Ibn Abbas also divided the foot into six distinct parts: calcaneus (Al‐Aqub), talus (Al‐Ka’ab), navicular (Al‐Zawraqi), four cuneiforms plus cuboid described under one name (Al‐Rasg), five metatarsals (Al‐Amshat), and five toes (Salamiat). Why then, do none of these anatomical structures bear his name?
Ibn Sina is also of particular importance to the subject of human anatomy, especially given that his magnum opus — Al Qanoon Fi Al Tibb (The Canon of Medicine or simply the Canon) became the authority on human anatomy for over 800 years replacing the word done by the ancient Greco-Roman physician-philosopher Aelius Galenus (or simply Galen 129 AD — 200 / 216 AD) ,who was famous for his work on the physiology of the circulatory system and who retains the naming rights to the GCV or Great Cerebral Vein, also affectionately known as the Great Vein of Galen. (An interesting fact is that Al Razi was the first to describe how the recurrent laryngeal nerve, a branch of the Vagus nerve, operates as both a mixed sensory and motor nerve).
Completed in 1025 AD, Ibn Sina’s Canon was the world’s first encyclopedia of medicine collected in five books. Its encyclopedic content, systematic arrangement, and its combination of Galen’s medicine with Aristotle’s science and philosophy helped the Canon become a mainstay of European scholastic medicine. Christian medical scholars started to use the Canon in the 13th century, with top Latin university courses implementing the text from the 14th century onwards. The Canon’s influence declined in the 16th century as a result of humanists’ preference in medicine for ancient Greek and Roman authorities over Arabic authorities, which is probably one of the reasons why no anatomical structures are named after Muslim or Arab anatomists.
A Prayer Spot: The Prophet Mohammad’s (PBUH) Protuberance

In Verse 29 of Surat Al Fath (“The Victory”), Allah S.W.T mentions that “their mark is on their faces from the trace of prostration”

سِيمَاهُمْ فِي وُجُوهِهِمْ مِنْ أَثَرِ السُّجُودِ) الفتح: 29)
Indeed, a small dark mark is left on the forehead of the pious as a result of the pressure applied by the frontal bone (Al‐Jabha) of the skull and frontalis muscle from prostrating at least 34 times a day (assuming the 17 raka’a that make up the obligatory five daily prayers).
This constant pressure leaves a permanent mark on the stratum corneum, the outer layer of the skin whose function is to prevent the interior skin tissues from stress and damage. It is important to note that the skin (the largest organ in the human body) has many layers from outside in including the stratum corneum, stratum lucidum (hands and feet), stratum granulosum, stratum spinosum, and stratum germinativum.
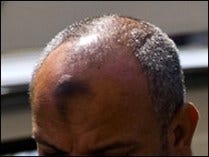
Unfortunately, there is no mention of this phenomenon in scientific anatomy journals despite its prominence amongst the almost two billion Muslims on this planet. As an amateur anatomist, I motion to label this prominent prayer’s spot as the Prophet Mohammad’s (PBUH) Protuberance (PMP). The PMP can be so pronounced creating a callus thick that actually protrudes from the forehead. And before the anatomical purists' motion to complain that skin anomalies are not named in the Terminologia Anatomica, may I simply point to that famous landmark of the integumentary system — Darwin’s Tubercle. (Interestingly enough, it is documented that Darwin himself named the anatomical representation of this congenital ear condition the Woolnerian tip, after Thomas Woolner, a British artist who had depicted it in one of his sculptures).
In terms of medical relevance, the PMP can be a type of acanthosis nigricans, which is a sign of insulin resistance usually from type 2 diabetes, a chronic disease that is becoming all too common in Muslim majority nations.
Razouki’s Dorsal Callus
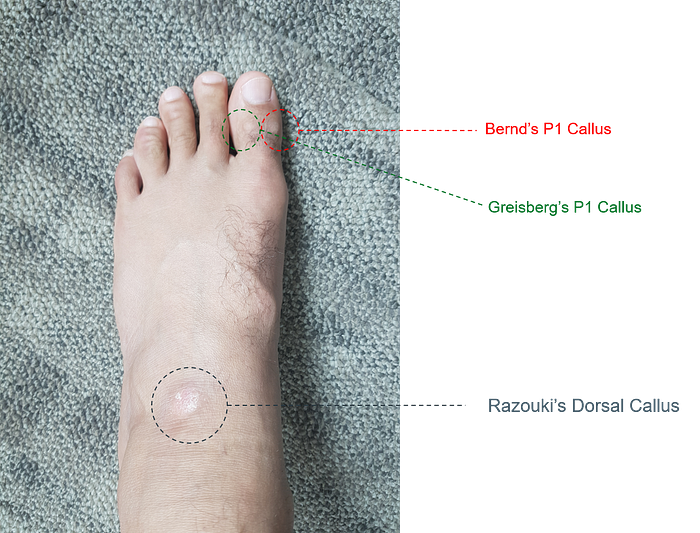
Keeping in line with the “first to document, first to claim” rationale, the author would also like to claim naming rights to three other prominent skin calluses found in Muslim populations, this time on the opposite side of the corpus humanum — the left foot (see above). The smaller two callus’ have been named after prominent professors Paulette Bernd and Justin Greisberg of Columbia University, who supported in the scoping of this study. Further anthropometric research is currently under discussion.
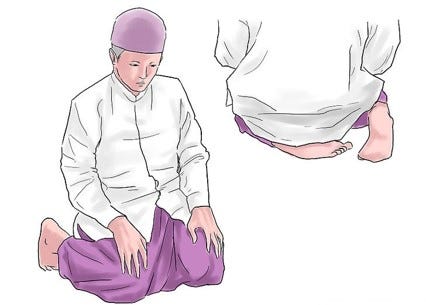
These calluses usually present unilaterally (on one side of the body), more specifically on the left foot, due to the contortion of the lower extremities during the final part of the Muslim act of prayer. This seated positioning results in pressure from the tarsal bones (cuneiforms or Al‐Rasg + navicular or Al‐Zawraqi) and the quadratus plantae muscle, creating the prominent RDC or Razouki Dorsal Callus. Related pivoting pressure is applied from the joints of the P1 phalange and metatarsal bones as seen in the below diagram resulting in the other two smaller calluses.
Beyond the anatomical, the documentation of these calluses is particularly important, again given the prominence of Diabetic Foot Ulcer in Muslim majority countries, especially since close to 15% of patient with diabetes develop a foot ulcer. The diabetic foot ulcer also precedes 84% of all diabetes-related lower-leg amputations.
References
- Finger, Stanley (2001). Origins of Neuroscience: A History of Explorations Into Brain Function. Oxford University Press. p. 177. ISBN 978–0–19–514694–3.
- A.C. Brown, Jonathan (2014). Misquoting Muhammad: The Challenge and Choices of Interpreting the Prophet’s Legacy. Oneworld Publications. p. 12. ISBN 978–1780744209.
- McGinnis, Jon (2010). Avicenna. Oxford: Oxford University Press. p. 227. ISBN 978–0–19–533147–9.
- “The great systematizers”. U.S. National Library of Medicine. Retrieved 12 October 2015. the title Qanun, meaning ‘canon’ or ‘codes of law’,
- Nasser, Mona; Tibi, Aida; Savage-Smith, Emilie (2009). “Ibn Sina’s Canon of Medicine: 11th century rules for assessing the effects of drugs”. Journal of the Royal Society of Medicine. PMC. 102 (2): 78–80. doi:10.1258/jrsm.2008.08k040. PMC 2642865. PMID 19208873.
- Mohammadali M. Shojaa, R. Shane Tubbsb, Marios Loukasc, Majid Khalilid, Farid Alakbarlie, Aaron A. Cohen-Gadola; Tubbs, RS; Loukas, M; Khalili, M; Alakbarli, F; Cohen-Gadol, AA (29 May 2009). “Vasovagal syncope in the Canon of Avicenna: The first mention of carotid artery hypersensitivity”. International Journal of Cardiology. Elsevier. 134 (3): 297–301. doi:10.1016/j.ijcard.2009.02.035. PMID 19332359.
- Siraisi, Nancy (1987). Avicenna in Renaissance Italy : the Canon and medical teaching in Italian universities after 1500. Princeton, NJ: Princeton University Press.
- Yazdanpanah, L; Nasiri, M; Adarvishi, S (15 February 2015). “Literature review on the management of diabetic foot ulcer”. World Journal of Diabetes. 6 (1): 37–53. doi:10.4239/wjd.v6.i1.37. PMC 4317316. PMID 25685277.
- Brem, H.; Tomic-Canic, M. (2007). “Cellular and molecular basis of wound healing in diabetes”. Journal of Clinical Investigation. 117 (5): 1219–1222. doi:10.1172/JCI32169. PMC 1857239. PMID 17476353.
- Turns M (2013). “Diabetic foot ulcer management: the podiatrist’s perspective”. Br J Community Nurs. Suppl: S14, S16–9. PMID 24796080.